Composite risk of having a fatal cardiac event.

Current guidelines on the prevention of cardiovascular disease (CVD) focus on lifestyle interventions and the optimal control of traditional cardiovascular risk factors such as hypercholesterolemia, hypertension, diabetes and smoking. However, the guidelines also highlight the need to integrate inflammatory status into cardiovascular disease risk assessment.
Risk scores such as QRISK3 score, ESC SCORE2, and ASCVD Pooled Cohort Equation, use traditional cardiovascular risk factors to calculate risk of atherosclerotic cardiovascular disease.
CCTA is traditionally used to augment these clinical risk scores by identifying patients with obstructive coronary artery disease.
However, twice as many cardiac deaths occurred in patients traditionally classified as low risk.*
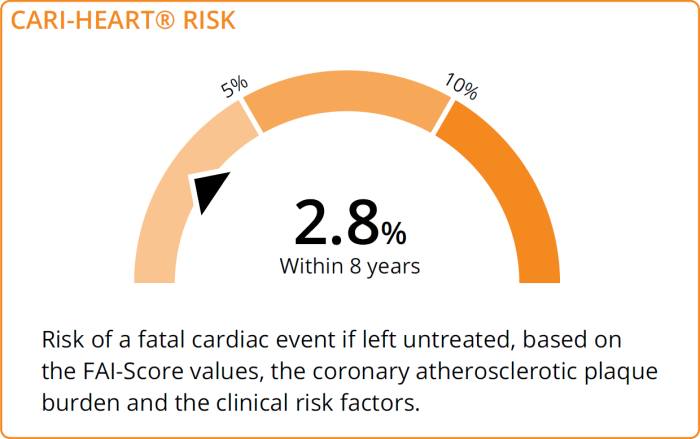
CaRi-Heart® Risk provides an individualised absolute risk of a fatal cardiac event within the next 8 years, incorporating:
CaRi-Heart Risk Score is trained and validated on over 10,000 patients. Results from the ORFAN study revealed that CaRi-Heart Risk reclassified ~30% of patients to a higher-risk category and ~10% of patients to a lower-risk category, and changed treatment recommendation for 45% of patients.
Watch this presentation by Prof. Keith Channon, Chair of Cardiovascular Medicine at the University of Oxford and Chief Medical Officer at Caristo Diagnostics, demonstrating how CaRi-Heart Risk Score and FAI-Score, transform risk stratification and management of patients with coronary artery disease.